Online first
Current issue
Archive
Special Issues
About the Journal
Publication Ethics
Anti-Plagiarism system
Instructions for Authors
Instructions for Reviewers
Editorial Board
Editorial Office
Contact
Reviewers
All Reviewers
2025
2024
2023
2022
2021
2020
2019
2018
2017
2016
General Data Protection Regulation (RODO)
RESEARCH PAPER
Evaluation of occupational exposure to wood dust among sawmill workers within the Gert Sibande District Municipality, South Africa
1
Department of Life Sciences, Central University of Technology, Free State, Bloemfontein, South Africa
2
Department of Clinical Sciences, Central University of Technology, Free State, Bloemfontein, South Africa
Corresponding author
Moeletsi Rathipe
Central University of Technology, Free State, 9 POWER STREET, ERMELO, Private Bag X20539, , Bloemfontein, South Africa
Central University of Technology, Free State, 9 POWER STREET, ERMELO, Private Bag X20539, , Bloemfontein, South Africa
Ann Agric Environ Med. 2022;29(4):483-488
KEYWORDS
TOPICS
ABSTRACT
Introduction and objective:
Wood dust is regarded as one of the human carcinogen based on an increased risk of nasal and sinonasal cancer. This study was conducted in two sawmills to measure and determine the time-weighted average (TWA) exposure level to wood dust, and compare the results with the South African occupational exposure limit (OEL).
Material and methods:
Personal and area respirable and total inhalable wood dust samples were collected using calibrated Giliair-3 personal air sampling pump (Sensidyne, USA). Data was analysed using Microsoft Office Excel 2019 Analysis Tool Pak for a summary of descriptive statistics. Both the geometric means and standard deviation as well as the minimum and maximum values were calculated.
Results:
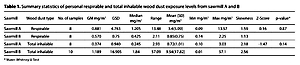
The geometric mean = GM (geometric standard deviation = GSD) for personal respirable wood dust exposure at sawmill A was 0.9(4.8) mg/m3 while at sawmill B – 0.57(0.75) mg/m3. The GM(GSD) for personal total inhalable wood dust exposure at sawmill A was 0.37(0.94) mg/m3 while at sawmill B – 1.19(16.91) mg/m3. Besides that, the GM(GSD) for area respirable wood dust at sawmill A was 0.13(0.09) mg/m 3 , while at sawmill B – 0.8(0.6) mg/m3. Likewise, the GM(GSD) for area total inhalable wood dust at sawmill A was 0.13(0.16) mg/m3 while at sawmill B – 0.54(0.55) mg/m3 .
Conclusions:
Results for the majority of samples were below the OEL. Workers smoking tobacco or cigarettes should be encouraged to stop smoking since smoking, especially when associated with exposure to wood dust, may increase the risk of respiratory health symptoms
Wood dust is regarded as one of the human carcinogen based on an increased risk of nasal and sinonasal cancer. This study was conducted in two sawmills to measure and determine the time-weighted average (TWA) exposure level to wood dust, and compare the results with the South African occupational exposure limit (OEL).
Material and methods:
Personal and area respirable and total inhalable wood dust samples were collected using calibrated Giliair-3 personal air sampling pump (Sensidyne, USA). Data was analysed using Microsoft Office Excel 2019 Analysis Tool Pak for a summary of descriptive statistics. Both the geometric means and standard deviation as well as the minimum and maximum values were calculated.
Results:
The geometric mean = GM (geometric standard deviation = GSD) for personal respirable wood dust exposure at sawmill A was 0.9(4.8) mg/m3 while at sawmill B – 0.57(0.75) mg/m3. The GM(GSD) for personal total inhalable wood dust exposure at sawmill A was 0.37(0.94) mg/m3 while at sawmill B – 1.19(16.91) mg/m3. Besides that, the GM(GSD) for area respirable wood dust at sawmill A was 0.13(0.09) mg/m 3 , while at sawmill B – 0.8(0.6) mg/m3. Likewise, the GM(GSD) for area total inhalable wood dust at sawmill A was 0.13(0.16) mg/m3 while at sawmill B – 0.54(0.55) mg/m3 .
Conclusions:
Results for the majority of samples were below the OEL. Workers smoking tobacco or cigarettes should be encouraged to stop smoking since smoking, especially when associated with exposure to wood dust, may increase the risk of respiratory health symptoms
ACKNOWLEDGEMENTS
The authors express their thanks to the managements of the sawmills for granting permission to conduct the study, as well as to the workers for their participation in
the study.
REFERENCES (56)
1.
Alwis KU. Occupational exposure to wood dust. Department of Public health and community medicine at the faculty of medicine. New South Wales, Australia: University of Sydney; 1989.
2.
Global Environment Fund report. Africa will import not export wood. 2013, http://www.criterionafrica.com....
3.
National Toxicology Program (NTP). Wood dust: report on carcinogens. 14th Edition. Triangle Park, NC: NIEHS; 2016.
4.
IARC. Wood dust and formaldehyde, IARC monographs on the evaluation of carcinogenic risks to humans. Lyon, France: WHO; 1995.
5.
IARC. Metal, arsenic, dust and fibres. IARC monographs on the evaluation of carcinogenic risks to humans. Lyon, France: WHO; 2012b.
6.
Kauppinen T, Vincent R, Liukkonen T, et al. Occupational exposure to inhalable wood dust in the member states of the European Union. Ann of Occup Hyg. 2006; 50: 549–561.
7.
Alwis KU, Mandryk J, Hocking AD. Exposure to biohazards in wood dust: bacteria, fungi, endotoxins, and (1›3)-ß-D-glucans. Occup Environ Hyg. 1999;14:598–608.
8.
Alwis KU, Mandryk J, Hocking AD, at al. Dust exposures in the wood processing industry. Am Ind Hyg Assoc J. 1999; 60: 641–646.
9.
Mandryk J, Alwis, KU, Hocking AD. Work-related symptoms and dose-response relationships for personal exposures and pulmonary function among Woodworkers. Am J of Ind Med. 1999;35:481–490.
10.
Lee T, Harper M, Slaven JE, et al. Wood dust sampling: field evaluation of personal samplers when large particles are present. Ann Occup Hyg. 2011;55:180–191. doi:10.1093/annhyg/meq075.
11.
Brown JS, Gordon T, Price O, et al. Thoracic and respirable particle definitions for human health risk assessment. Part Fibre Toxicol. 2013;10:12. doi: 10.1186/1743-8977-10-12.
12.
Demers PA, Teschke K, Davies HW, et al. Exposure to dust, resin acids, and monoterpenes in softwood lumber mills. Am Ind Hyg Assoc J. 2000;61:521–8.
13.
Teschke K, Demers PA, Davies HW, et al. Determinants of exposure to inhalable particulate, wood dust, resin acids, and monoterpenes in a lumber mill environment. Ann of Occup Hyg. 1999b;43:247–255.
14.
Wenzel FJ, Emanuel DA. The epidemiology of maple bark disease. Arch Environ Health. 1967;14:385–389.
15.
Terho EO, Husman K, Kotimaa M, et al. Extrinsic allergic alveolitis in a sawmill worker. A case report. Scand J Work Environ Health. 1980;6:153–157.
16.
Van Assendelft AHW, Raitio M, Turkia V. Fuel-chip induced hypersensitivity pneumonitis caused by Penicillium species. Chest. 1985;87:394–396.
17.
Eduard W, Sandven P, Levy F. Relationships between exposure to spores from Rhizopus microsporus and Paecilomyces variotii and serum IgG antibodies in wood trimmers. Int Arch Allergy Immunol. 1992; 97:274–282.
18.
Halpin DMG, Graneek BJ, Lacey J, et al. Respiratory symptoms, immunological responses, and aeroallergen concentrations at a sawmill. Occup Environ Med. 1994a;51:165–172.
19.
Halpin DMG, Graneek BJ, Turner-Warwick M, et al. Extrinsic allergic alveolitis and asthma in a sawmill worker: Case report and review of the literature. Occup Environ Med. 1994b;51:160–164.
20.
Mackiewicz B, Dutkiewicz J, Siwiec J, et al. Acute hypersensitivity pneumonitis in woodworkers caused by inhalation of birch dust contaminated with Pantoea agglomerans and Microbacterium barkeri. Ann Agric Environ Med. 2019; 26: 644–655.
21.
Wójcik-Fatla A, Mackiewicz B, Sawczyn-Domańska A, et al. Timber-colonizing gram-negative bacteria as potential causative agents of respiratory diseases in woodworkers. Int Arch Occup Environ Health. 2022;95:1179–1193.
22.
Belin L. Sawmill Alveolitis in Sweden. Int Arch Allergy Appl Immunol. 1987;82:440–443.
23.
Land CJ, Hult K, Fuchs R, et al. Tremorgenic mycotoxins from Aspergillus fumigatus as a possible occupational health problem in sawmills. Appl Environ Microbio.1987;53:787–790.
24.
Rylander R. Organic dusts and lung reactions—exposure characteristics and mechanisms for disease. Scand J Work Environ Health. 1985; 11:199–206.
25.
Kulkarni CM, Karigoudar MH, Aithala M. Measurement of wood dust particle size by optical microscopy technique and long-term effect on sawmill workers: A random study. Asian J Phar Clin Res. 2016;9:308–311.
26.
Szewczyńska M, Pośniak M. Assessment of occupational exposure to wood dust in the Polish furniture industry. Pub Med. 2017; 68:45–60.
27.
Health and Safety Executive. MDHS 14/3: General Methods for sampling and gravimetric analysis of respirable and inhalable dust. Sudbury, Suffolk: Health and Safety Executive; 2000. Reviewed (MDHS 14/4: General method for sampling and gravimetric analysis of respirable, thoracic and inhalable aerosols. Sudbury, Suffolk: Health and Safety Executive; 2015).
28.
NIOSH. Particulates not otherwise regulated, total 0501. 5th Edition. Cinthinathi, Ohio: NIOSH; 1989.
29.
Sensidyne. Gilian Gillibrator 2 calibration system operations and service manual. Florida, USA: Sensidyne, LP; 2008. Document No. 850190M.
30.
Sensidyne. Gilair-3 & Gilair-5 air sampling systems operational manual. Florida, USA: Sensidyne, LP; 2012. Document No.:360-0040-01 (Rev R).
31.
Davies B, Henderson J. W501-student manual measurement of hazardous substance. Australia: University of Wollongong; 2009.
32.
Drolet D, Beauchamp G. Sampling guide for air contaminants in the workplace. 8th Edition. Québec: IRSST; 2013.
33.
Eller PM, Cassinelli ML. NIOSH manual of analytical methods. 4th Edition. Cincinnati, Ohio: Diane Publishing; 1994.
34.
Leidel NA, Busch KA, Lynch JR. Occupational exposure sampling strategy manual. Cincinnati, USA: NIOSH; 1977.
35.
Harmse L. Implementing an air monitoring programme. Occup Health South Africa. 2000; 6:14–17.
36.
Ministry of Human Resources. Guidelines on monitoring of airborne contaminant for chemicals hazardous to health under the occupational safety and health (use and standard of exposure of chemicals hazardous to health) regulations. Malaysia: DoSH; 2000.
37.
South Africa. Regulations for hazardous chemical substances GN. No.1179 of 25 August 1995. Pretoria: Government printer; 1995. (Repealed by Regulation for Hazardous Chemical Agents GN No. R. 280 of 29 March 2021).
38.
Osuchukwu NC, Osuchukwu EC, Eko JE, et al. Occupational exposure to wood dust in Calabar municipality, cross river state, Nigeria. Int J Sci Res. 2015; 4: 23–29.
39.
Kalliny MI, Brisolara JA, Glindmeyer H, et al. A survey of size-fractionated dust levels in the US wood processing industry. J Occup Environ Hyg. 2008;5:501–510.
40.
Löfstedt H, Hagström K, Bryngelsson IL, et al. Respiratory symptoms and lung function in relation to wood dust and monoterpene exposure in the wood pellet industry. Ups J Med Sci. 2017;122:78–84. doi: 10.1080/03009734.2017.1285836.
41.
Cormier V, Merlaux A, Duchaine C. Respiratory health impact of. working in sawmills in eastern Canada. Arch Environ Health. 2000; 2000, 55: 424–430.
42.
Chan-Yeung M, Giclas PC, Henson PM. Activation of complement by plicatic acid, the chemical compound responsible for asthma due to western red cedar (Thuja plicata ). J Allergy Clin Immun. 1980;65: 333–337.
43.
Ahman M, Holmström M, Cynkier I, et al. Work related impairment of nasal function in Swedish woodwork teachers. J Occup Environ Med. 1996;53:112–117.
44.
Hessel PA, Herbert FA, Melenka LS, et al. Lung health in sawmill workers exposed to pine and spruce. Chest. 1995;108:642–646.
45.
Schlünssen V, Schaumburg I, Taudorf E, et al. Respiratory symptoms and lung function among Danish woodworkers. J Occup Environ Med. 2002a; 44: 82–98.
46.
Holness DL, Sass-Kortsak AM, Pilger CW, et al. Respiratory function and exposure-effect relationships in wood dust-exposed and control workers. J Occup Environ Med. 1985;27:501–506.
47.
Mandryk J, Alwis KU, Hocking AD. Effects of Personal Exposures on Pulmonary Function and Work-related Symptoms Among Sawmill Workers. Ann Occup Hyg. 2000;44:281–289.
48.
Holmstrom M, Wilhelmsson B. Respiratory symptoms and pathophysiological effects of occupational exposure to formaldehyde and wood dust. Scand J Work Environ Health. 1988;14:306–311.
49.
Goldsmith DF, Shy CM. Respiratory health effects from occupational exposure to wood dusts. Scand J Work Environ Health. 1988a;14:1–15.
50.
Goldsmith DF, Shy CM. An epidemiologic study of respiratory health effects in a group of North Carolina furniture workers. J Occup Med. 1988b;30:959–965.
51.
Andersen HC, Andersen I, Solgaard J. Nasal cancers, symptoms and upper airway function in woodworkers. Brit J Ind Med. 1977;34:201–217.
52.
Pisaniello DL, Connell KE, Muriale L. Wood dust exposure during furniture manufacture results from an Australian survey and considerations for threshold limit value development. Am Ind Hyg Assoc J. 1991;52:485–492.
53.
Jacobsen G, Schlünssen V, Schaumburg I, et al. Longitudinal lung function decline and wood dust exposure in the furniture industry. Eur Respir J. 2008;31:334–42.
54.
Hall AH, Teschke K, Davies H, et al. Exposure levels and determinants of softwood dust exposures in BC lumber mills, 1981–1997. Am Ind Hyg Assoc J. 2002;63:709–14.
55.
Scarselli A, Binazzi A, Ferrante P, et al. Occupational exposure levels to wood dust in Italy, 1996–2006. Occup Environ Med. 2008;65:567–574.
56.
Tobin EA, Ediagbonya TF, Okojie OH, et al. Occupational exposure to wood dust and respiratory health status of sawmill workers in South-South Nigeria. J Pollut Eff Cont. 2016; 4: 154. doi:10.4172/2375-4397.1000154.
Share
RELATED ARTICLE
| eISSN: | 1898-2263 |
| ISSN: | 1232-1966 |

Generation of the DOI (Digital Object Identifier) - task financed under the agreement No NrRCN/SP/0532/2021/1 by the Minister of Science and Higher
© 2006-2026 Journal hosting platform by Bentus
We process personal data collected when visiting the website. The function of obtaining information about users and their behavior is carried out by voluntarily entered information in forms and saving cookies in end devices. Data, including cookies, are used to provide services, improve the user experience and to analyze the traffic in accordance with the Privacy policy. Data are also collected and processed by Google Analytics tool (more).
You can change cookies settings in your browser. Restricted use of cookies in the browser configuration may affect some functionalities of the website.
You can change cookies settings in your browser. Restricted use of cookies in the browser configuration may affect some functionalities of the website.